

This happened to my wife and I recently.
We came for a visit and her usual doctor wasn’t available. This new doctor flat out said, “I didn’t get a chance to read your medical history so tell me what’s going on.” My wife was confused, because this was her third visit to check her hormone levels. it wasn’t a checkup, but a followup.
And this doctor proceeds to not understand any of this, as she keeps asking her questions about why she might be there, instead of spending two minutes reading the medical history.
My wife ends up crying while Im sitting in the corner begging my wife we should just leave because shes not getting anything from this doctor.
Like George Carlin said, somewhere there is the worst doctor and someone has an appointment with them tomorrow!

What do you call the person who was last in class at medical school?
…
…
Doctor
Having been a paramedic for many years, I’ll take the 80% med student over the no bedside manner, no common sense, overly bookish student who can only think about what the book told them.
This is the third time I’ve read this comment today. I hope Joe Pesci or the sun aren’t trying to tell me something.

Medical clinics are often overbooked, like airports. This is why they give you an appointment time that is generally thirty minutes early. ONE late person fucks the entire day’s schedule after their appointment time, that’s how tightly management insists on arranging it. Even the extra time slots of the past are being booked or even double booked in advance of the day. Docs are often given 10-15min per patient. Those other rooms you see in the hall? There are patients inside waiting for doc to go down the line, as staff keeps refilling those rooms down the line as the doc finishes. You think there’s time to read between? Oh you sweet summer child. That’s not on docs, that’s on corporate. Whatever company logo is stamped on the clinic and also on the nearby hospital, they’re the ones making it happen that way. Why? More patients crammed into each day means more $$$. Quantity over quality. Clinic docs are also paid by patient encounter. So this works together to arrange what we in healthcare commonly call a clusterfuck.
.
This is the part that’s probably messing with you most. And it likely won’t change. In medical, the assessment is sacrosanct. And your own. You MUST do it yourself. You don’t just go with the assessment of the first person to do one and never check again, you always check again. Always. Every visit. A lot can change in half a day. A day. A week. A month. And the quality of assessment changes with each person. Each person. Medical isn’t robots, it’s people, and most data collection happens through people. Each medical staff, doc or NP or RN or PA, gets their own assessments before they begin, unless they’re utter garbage at their jobs. This doctor never assessed you before, which means, they MUST assess you now, per their licensing. Also, a good chunk of what’s in the chart is old news. What’s right in front of you contains the best data about the patients present state. And the speed at which a clinic is to move from patient to patient, 2 min to read a chart isn’t part of the schedule. Even logging in these days can take half that 10min time slot due to old crappy computers. Sure stuff like moms medical history, what tests you’ve had already, and meds (pharmacies e-record talks to your medical e-record these days) is current, but your present state changes day to day and asking YOU what’s happening today is usually best practice and the most accurate. There’s no day prep time to a clinic day and no one takes “homework” home after work. It’s hit the ground running and just start diving into appointments. When the doc knows the patient already ofc this goes more smoothly because the doc knows the bigger picture. That’s why there’s an assigned doc for each patient.
.
All the NPs being trained makes the process more difficult. Heavy revolving door there as they do their version of residency and then poof they’re gone to find their actual job.
.
Wait until you’re admitted to a hospital from an emergency room, you’ll be in for a real treat. /s.
For-profit medicine is a cruelty unlike any other. The United States government’s embrace of this system is truly abhorrent.
Somewhere, dunno where, there is a country where doctors in state medical institutions make less than me, get bullied by superiors daily, deal with all kind of bureaucratic paper fuckery, and yet show the heroism of not leaving that work for greener pastures in private medical institutions which pay normal. And they are conscious of that. Cause sometimes lonely old people, or clueless\lost\just poor people, or someone unprepared, need help.
Your system might not be good, but if you are thinking of building some other one, please think how it’s going to make doctor’s pay proportional to their value for the society, without tanking the rest of said society.
It’s a valid strategy to ask the patient to recap what brings them to the clinic. It’s very common to hear a different story from the one in the booking system or in the medical history. I’m not sure about the system were you live but medical history often takes waaaaaaaaaay more than 2 min to read up on. Maybe the last visit was recorded and had yet to been transcribed? Those can be a pain to listen to. It feels very reasonable that the doctor didn’t have time to read up on your history if they were covering for a sick/unavailable colleague.
I would 100% prefer a doctor that is upfront about not knowing my medical history over a (more commonly occurring) dumbass pretenting to know it.
It’s regrettable that your doctor made you feel neglected. Fault them for that, not the questions.
Edit: *recorded as in dictated!

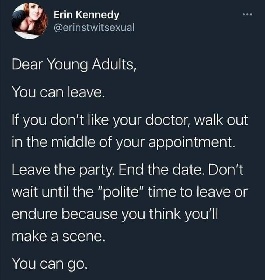
this should be made more clear to all patients of all ages, throughout life. they can’t force you to do anything, or do anything to you that you don’t want them to do
Nope. In medical, you educate and advise, the patient decides. Then it’s documented and you move on to the next patient.
In diabetes this is often seen as a foot that is now getting amputated after years of noncompliance with medical advice, but again, all you can do is educate. People decide their own actions for themselves.
As long as you don’t mind burning bridges*

An objectionable acquaintanceship may be reconcilable.
The person leaving might not be objective in a situation and might realize that they miss the metaphorical bridge.
A person you dislike might be a valuable resource in other ways beyond social (especially in the referenced example of a medical professional).
Things change. For example:
- burn a bridge at a company w/ a terrible boss - boss leaves and is replaced by a much better manager, but you have no shot because HR is still pissed at you
- burn a bridge w/ a date - you end up working with that date and they remember how rude you were and end up making things suck for you
- burn a bridge w/ a doctor - doctors tend to be friends w/ other doctors, so other doctors may choose to not bring you on
That doesn’t mean you should let people walk all over you, it just means a little professionalism goes a long way. If you can’t stand your boss, give them a reasonable notice that you’re leaving. If your date is late, send them a text saying something came up and can no longer wait for them. If your doctor sucks, thank them for their time and ask for a referral for a second opinion, or if they take too long to see you, tell the front staff to cancel your appointment on your way out.
You don’t have to put up with nonsense, but you should handle it as gracefully as you can, because it doesn’t cost you much and you never know if it’ll end up mattering.


I don’t like my dentist. But every other dentist has an 18 month waiting list. So I deal with the dentist I hate.

{kind=link}
{kind=link}